
A Strategic Direction for the New Department of Senior Citizens Welfare

In a quiet village in Pathanamthitta, a 78 year-old woman cooks for one. Her two children live in Toronto and Doha. Her husband died four years ago. The pension comes on time. The neighbours look in now and then. By every official measure, she is doing fine. Most evenings, though, she sits alone with the television on for company, takes her seven medicines in an order she has half-forgotten, and waits for a phone call. She is not poor, not abandoned. She is also not, in any honest sense, doing well.
There are versions of her in almost every panchayat in Kerala. The configurations vary: a daughter-in-law nearby, a hired caregiver of uncertain training, a son in Bangalore who pays for everything and visits at Onam. The underlying reality does not. We have built a society in which living to a great age has become ordinary, and the conditions that would make that long life a good one have not caught up.
This is the inheritance of Kerala's own success. Literacy went up, fertility came down, and life expectancy rose. We built one of the densest public health systems in the Global South, and a community palliative care movement that the world now studies. The reward is a population ageing faster than in any other part of India. The elderly will account for close to a quarter of Kerala's population by 2036, and in some panchayats, that line has already been crossed.
The state, officially referred to as Keralam in recent government communications, has just taken a significant step: it has become the first state in India to establish a dedicated department for senior citizens. The Department of Senior Citizens Welfare was established by Government Order in the first Cabinet meeting of the new UDF government under Chief Minister V.D. Satheesan. The Department's formal mandate is to formulate and implement new welfare schemes for the elderly, and to coordinate and execute existing ones.
This is not a routine administrative reorganisation. It is the moment when Kerala has to decide whether ageing will be addressed as a welfare problem or as a development frontier. The argument in this paper is that the Department's name sits firmly in the old paradigm, Senior Citizens Welfare, and its practice must be larger than its name.
Done well, the Department can show how the state reorganises itself for a different demographic future. Done badly, it will be one more office in which good intentions are filed and forgotten.
The Department works alongside the Kerala State Senior Citizens Commission, established under the Kerala State Senior Citizens Commission Act, 2025. The Commission is a statutory rights body. The Department is the executive arm. Together, they are intended to form what a full Ministry would have been in a single institution.
What the demographics are actually saying
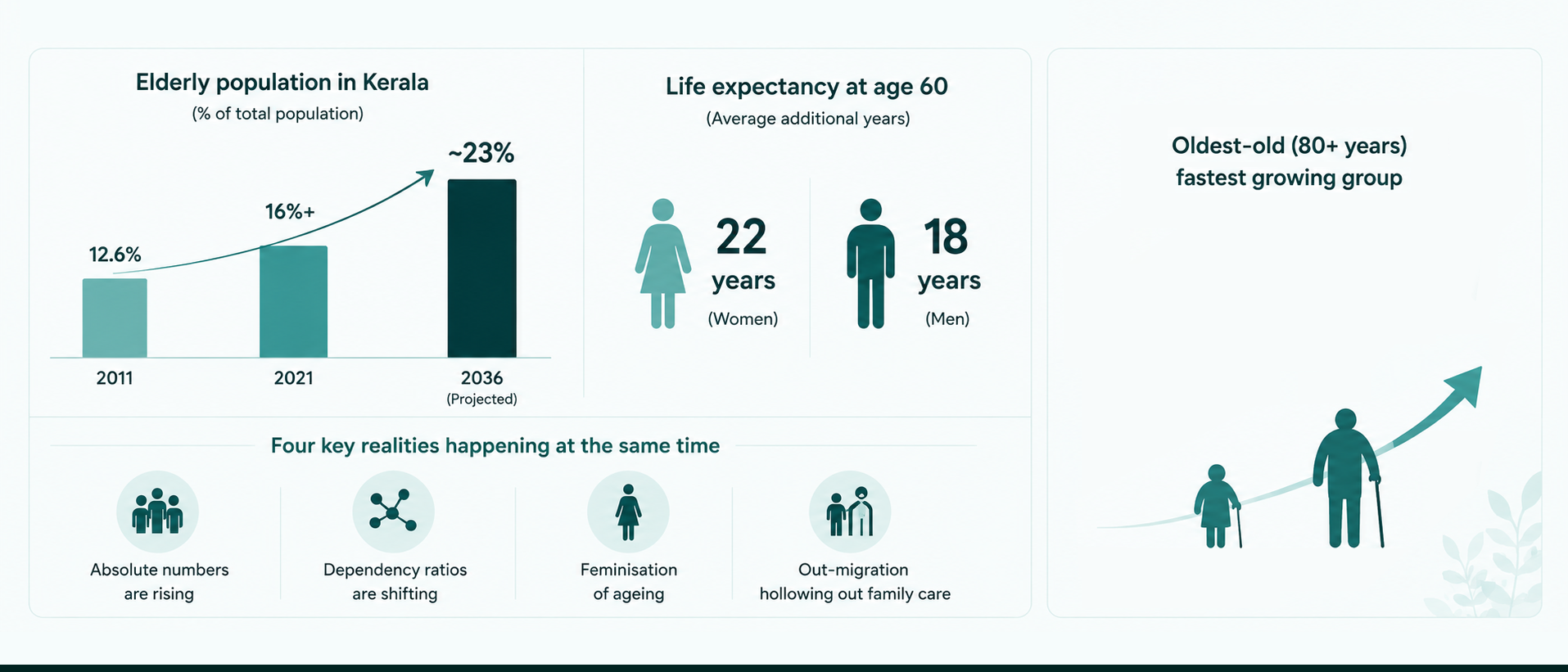
Kerala's elderly were 12.6% of the population in 2011, the highest share in India. By 2021, it had exceeded 16%. Projections take it to roughly 23 per cent by 2036. And once a Keralite reaches the age of 60, she can now expect to live another 22 years, on average, into her early 80s; a man, another eighteen, into his late seventies. Old age in Kerala is no longer a coda, but a third of a life. Within that category, the oldest-old, those above eighty, constitute the fastest-growing band and place the heaviest demand on long-term care.
The headline number hides four distinct things happening at the same time. Absolute numbers are rising. Dependency ratios are shifting. The feminisation of ageing, women outliving men by about five years and being far more likely to be widowed, alone, and outside any contributory pension, produces a particular kind of vulnerability. And out-migration has hollowed out family-based care because the adult children who once provided it now live elsewhere. A policy that treats ageing as a single phenomenon will fail on three of these four.
There are also deeper inequalities inside the averages: elderly Dalits and Adivasis, older persons with disabilities, and those in flood-prone areas with mobility limits. Any serious Department will have to track them separately.
There is still time, narrow but real. The demographic pressure will continue to build through the 2030s and 2040s. The next decade is when the institutions can be put in place. After that, the state will be running to catch up.
The cost of the system we have now
Elderly concerns today are scattered across Social Justice, Health, Local Self-Government, Finance, and a long list of mission programmes that rarely coordinate. Vayomithram, Sayamprabha, Sallapam, the palliative network, the pensions, the helplines: each does useful work, but they sit beside each other. Older persons routinely discover that the help they need exists somewhere, and that no one is responsible for putting it together for them.
The cost of that fragmentation is borne mostly privately by families. Out-of-pocket spending on elderly care is catastrophic. Chronic disease management runs through episodic private hospital visits and a steady drift towards larger pill burdens, with very little integration between specialists, primary care, and community follow-up. The system handles acute medical events reasonably well and almost everything else poorly.
Out-migration has weakened the family caregiver system before any formal one was ready to take over. Remittances support consumption. They do not provide daily care, manage medications, or supervise dementia. Women carry the heaviest end of this twice over: first as the elderly persons most often left alone, and then, while still middle-aged, as the family members expected to do unpaid caregiving even after entering the formal labour force. A gender-blind policy will be paid for by Kerala's women on both sides.
There is a conceptual failure, too, that has persisted across programmes and is now well documented in the international evidence base. Kerala's programmes still respond to ageing as a sequence of medical events: a fall, a stroke, a hospitalisation.
The WHO's Integrated Care for Older People (ICOPE) framework, which Kerala's health system has the infrastructure to adopt, makes it clear that functional ability, not just disease status, must be the central organising principle of care for older people. The ICOPE approach tracks six domains of intrinsic capacity: locomotion, cognition, vitality, sensory function, psychological wellbeing, and the capacity to carry out daily activities. It identifies declining trajectories early, enabling intervention before the clinical threshold is crossed.
The evidence from Japan's long-term care system, European models, and the WHO's own ICOPE trials now makes it clear that the sequence of acute events is the visible end of a much longer process of unattended decline. Frailty, malnutrition, depression, sensory loss, cognitive change: these build up quietly for years before anyone reaches a ward. By the time the system meets the person, the most important opportunities for intervention have passed.
And underneath all of it, the system does not really know what it is doing. There is no live, panchayat-level registry of older persons. Most administrative data treats the elderly as a single category, with no disaggregation by age band, sex, living arrangement, functional status, or vulnerability. Without continuous, disaggregated data, the state cannot target, cannot measure, and cannot correct.
What Japan figured out, and what travels
Japan worked through these questions a generation earlier. Some of what they learned travels straight to Kerala. Some of it needs adapting.
The clearest transferable lesson is that long-term care has to be socialised. Japan's Long-Term Care Insurance (LTCI), introduced in 2000, replaced the assumption that the family alone would bear the cost of care for dependents. The system has had to recalibrate several times as costs have risen, but it has changed what families expect and what older persons can demand.
Kerala cannot adopt national mandatory insurance overnight. It can, however, begin a Kerala Long-Term Care Fund as a pilot, drawing on state, employer, and self-employed premiums for those who can pay, a dedicated diaspora contribution, CSR, and means-tested co-payments. Start with home and community care for the moderately frail. Expand from there. The point is to start.
Second, care has to be organised at the community level, within roughly a thirty-minute reach of the older person's home. Japan calls this Community-Based Integrated Care. Kerala already has more of that architecture than it recognises: Kudumbashree, the palliative care movement, the ASHA cadre, the primary health centre network, a functioning three-tier local government, and a literate and digitally connected population. The job is to repurpose, train, fund, and connect these institutions, not to invent new ones.
Third, prevention pays. Falls prevention, frailty screening, hearing and vision, nutrition, social participation, and mental wellbeing. None of it produces ribbon-cutting moments. It is the difference between a population that lives healthily into its eighties and one that lives medicated and isolated into its eighties.
Where Japan does not transfer cleanly is technology. They leaned heavily on care robotics because they cannot fill their caregiver shortage through migration. Kerala is in a different position. We still have a substantial working-age population, particularly women, and the more urgent question is how to formalise and dignify caregiving as paid work. Technology supports that workforce; it does not replace it.
One Japanese caution worth carrying forward: even with all of their institutional architecture, social isolation among older persons has remained stubborn. Institutions help. The cultural work of staying connected cannot be outsourced to a programme.
The healthspan question

There is a wider international conversation, recently sharpened by cardiologist Eric Topol and echoed in the WHO's healthy ageing agenda, that is changing what success looks like. The conversation is about healthspan as distinct from lifespan.
Lifespan is how long a person lives. Healthspan is how long they live in good health, with cognitive engagement, physical capability, social connection, and some real agency over their own day. The two have come apart in most rich societies. They are coming apart in Kerala too.
What this changes is what the Department chooses to measure. Mortality rates and bed occupancy will be optimised to keep people alive. Healthy life expectancy, functional ability, and patient-reported wellbeing will optimise it for something quite different.
At the individual level, the reframe shifts the questions a care plan must ask: can the person move, are they cognitively engaged, do they have meaningful relationships, and do they have any say in how the day is spent?
These are not soft questions. Research now ties each of them to mortality and morbidity in measurable ways.
The woman in Pathanamthitta is not failing the medical system. The medical system is not, by its own lights, failing her. She is failing a system that has not yet decided whether her loneliness and her shrinking social world are clinical concerns or someone else's problem. The healthspan framing makes them clinical concerns. The Department can do the same.
The strategic shift Kerala must make
Underneath every recommendation in this paper is a shift in how the state thinks about ageing. It is worth setting that shift out plainly, because every piece of operational design depends on it.

Each pair has a budget, organisational, and workforce implication. The Department's design should be tested against this list. A programme that treats the older person as a passive recipient of medical events belongs to the old paradigm. A programme that treats her or him as someone whose physical, mental, and social wellbeing is a joint responsibility of the state and the community belongs to the new one.
Principles for the new Department
A few principles follow from the diagnosis and the shift.
Care must be person-centred, not scheme-centred. Older persons have multiple needs that cut across departments, and the test of the system is whether one person, walking through a single entry point, can have those needs met without navigating the bureaucracy themselves.
Care must be rights-based, not gift-based. Autonomy, dignity, non-discrimination, and protection from abuse should be enforceable entitlements, not expressions of governmental goodwill. The Kerala State Senior Citizens Commission Act, 2025, has begun this transition; the Department should consolidate it.
Care must be gender-responsive and inclusive. Ageing in Kerala is disproportionately female and disproportionately widowed, and impacts the most marginalised and vulnerable communities. A policy without a gender and inclusion lens will reproduce existing inequities on a greater scale, with more money behind them.
Prevention has to count as much as treatment, and home and community as much as hospital and institution. Hospital care should be the exception, mobilised when home and community can no longer meet the need.
The partnership has to be a Public-Private-Community Partnership (PPCP). The government sets standards, regulates providers, finances the universal floor, and ensures access for those who cannot pay. Non-state actors deliver much of the actual care and innovate at the edge. The Department's job is to make this partnership work, not to absorb everything into itself.
Underneath all of this, dignity is the test by which the system will eventually be judged.
A three-tier governance architecture
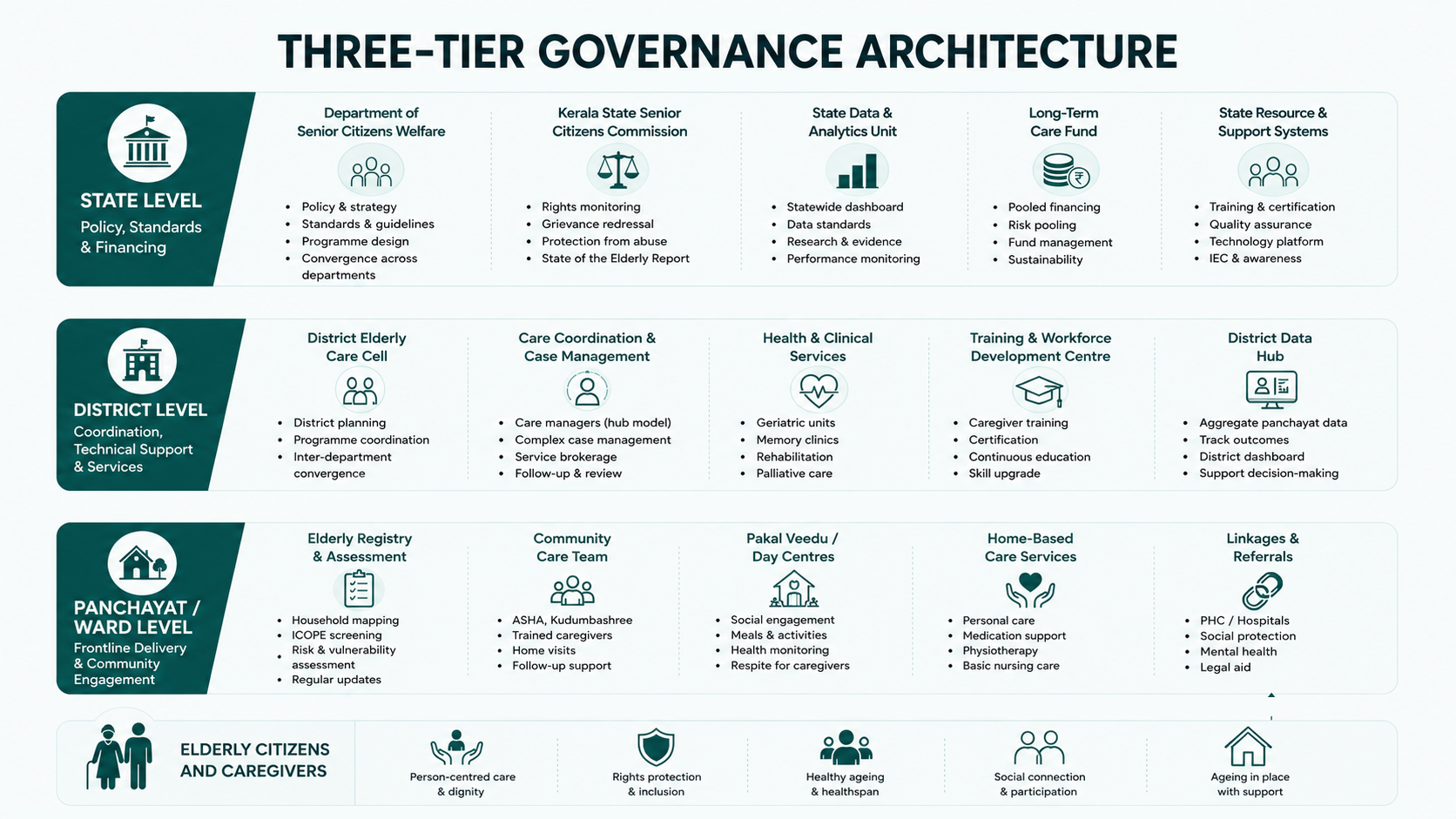
Kerala's three-tier local government system is unusually well suited to elderly care. The Department should build on it.
At the panchayat, municipality, and ward level sits the operational front line. Every panchayat and municipality needs a living elderly registry, not just demographic facts but functional status, living arrangements, caregiver presence, and identified risks. A designated elderly welfare officer should be responsible for it and for coordinating local services.
ASHAs and Kudumbashree members, with the right training, should administer regular ICOPE-style screening of intrinsic capacity. 'Pakal Veedu' day centres should provide structured social engagement, meals, basic health monitoring, and respite for family caregivers. Trained community caregivers, certified by a state-level workforce mission, should provide home-based care with proper supervision and pay.
At the district level sits the technical and coordinating layer. District hospitals need functioning geriatric units, memory clinics, rehabilitation capacity, and palliative care. Care coordinators, the Kerala equivalent of Japan's care managers, should be based here, handling complex cases that need ongoing brokerage across health, housing, and social protection.
A district training centre should run certification for community caregivers. District data systems should aggregate panchayat registries and monitor performance.
At the state level, the Department works in tandem with the Kerala State Senior Citizens Commission as the statutory rights body. The Department sets policy and standards, finances the Long-Term Care Fund, regulates providers across the public, private, and non-profit sectors, maintains statewide quality data, and ensures ageing is mainstreamed into every other ministry's planning.
The Commission handles rights monitoring, grievance redressal, and periodic State of the Elderly reporting.
A Department without an independent rights body becomes self-evaluating. A Commission without an operational counterpart stays purely advisory. The two are designed to reinforce each other. Together, they are the institutional architecture that, in its early years, substitutes for what a dedicated Ministry would have provided in a single political structure.
If a slogan helps: 'Age in place, care in community, protect with the state'.
Building blocks the Department should fund first
Within this architecture, certain investments determine whether the system actually works.
Data. A live panchayat-level elderly registry, with functional status indicators and continuous updating, linked to a state-level dashboard that the Department, the Commission, and the Planning Board can all read. No programme will outperform its data.
Workforce. A Care Workforce Mission with proper training, certification, supervision, and pay. Tens of thousands of new caregivers will be needed over the decade, mostly women, representing one of the state's most promising employment opportunities.
The Long-Term Care Fund. Begin small, with home and community care in two or three districts. Without sustainable financing, every other element of the architecture becomes a one-term initiative.
A dementia ecosystem. Dementia is the condition Kerala is least prepared for. Memory clinics in every district hospital, community Dementia Supporters trained through Kudumbashree and ASHA networks, at least one specialised facility per district, and a sustained public campaign that treats dementia as a societal responsibility rather than a family secret.
Age-friendly community infrastructure. Barrier-free public spaces, accessible transport, walkable neighbourhoods, dementia-friendly signage, and climate-resilient housing for older persons in flood-prone areas. Most of this falls under other departments; the Department for Senior Citizens Welfare serves in a coordinating role. An Age-Friendly Panchayat certification would create useful competition among local bodies.
Social participation. Senior citizens' clubs, intergenerational programmes with schools and colleges, lifelong learning models, structured volunteering, and Pravasi Care Circles for left-behind elderly in migrant households. The evidence on loneliness as a health risk is no longer in dispute. These are clinical interventions delivered in a social form.
Grief and mental health. Older persons in Kerala incur losses at a rate the system has yet to take seriously. Grief counselling, depression screening, and mental health support need to be available at the panchayat level, not only at district hospitals.
The economics, briefly
A properly designed elderly care system reduces costs currently being paid in less visible ways: hospitalisations from poorly managed chronic conditions, catastrophic out-of-pocket spending that operates as a regressive tax on middle-class families, the lost productivity of working-age adults, mostly women, who leave the labour force to care for parents, and the drift towards institutional care, the most expensive option in any system.
It also creates jobs. Kerala will need community caregivers, geriatric nurses, care coordinators, social workers, physiotherapists, and dementia specialists in numbers it does not have today. Properly paid and trained, this workforce becomes a significant employment sector.
And a formalised, well-regulated Kerala care workforce, trained to a recognised standard, will be in significant international demand. Done carefully, with an adequate domestic supply protected, this becomes a productive flow rather than another brain drain.
None of this is free. The Department will have to be candid with the Planning Board and the Finance Department about the early-year costs, before the savings begin to show up.
The ecosystem that the Department cannot do without
The government alone cannot do this. Kerala will need academic institutions for research and workforce development, NGOs and faith-based networks for community engagement, the private sector for assistive technology and diagnostic and care services, and a generation of social enterprises building integrated home and community care.
Initiatives such as Carenexs, working in the Kerala context on home-based care, family support, and the practical design of services around healthspan rather than survival, are the kind of community-rooted partner the Department will need to engage with seriously, regulate sensibly, and learn from.
The diaspora deserves particular mention. Non-resident Keralites have both a stake in the welfare of older persons at home and significant financial capacity. A dedicated channel for diaspora contributions, through the Long-Term Care Fund, philanthropic initiatives, or services for left-behind elderly in migrant households, would be both fiscally meaningful and politically powerful.
The diaspora is not a passive source of remittances. It is a potential partner with a clear role in the ecosystem.
Implementation realism
Kerala has a long history of announcing progressive social policies and then under-resourcing the administrative machinery that would deliver them. The Department faces a structural challenge that did not exist for a hypothetical Ministry: it will almost certainly be held by a Minister who also holds another portfolio.
That means the coordination authority the paper assumes, the capacity to push other departments into line, has to be built deliberately, not assumed.
The mechanisms that compensate for this are specific. The Department needs a ring-fenced annual ageing budget presented to the Legislative Assembly as a standalone line item, not subsumed under another department's head.
It needs formal coordination protocols with the Departments of Health, Social Justice, Local Self-Government, Finance, Labour, Housing, and Transport. Not memoranda of understanding that gather dust, but scheduled quarterly meetings with defined deliverables.
And it needs to route its statutory accountability through the Commission: the Commission's annual State of the Elderly Report to the Legislature is the check the Department cannot escape.
In year one, the work is foundational. Set up the Department's institutional structure. Strengthen the Kerala State Senior Citizens Commission by providing adequate funding and staffing. Begin the panchayat and municipal-level registry in a few pilot districts. Launch the Care Workforce Mission. Start design work on the Long-Term Care Fund. Establish the coordination mechanisms with line departments. Resist the temptation to announce too many programmes at once.
In years two and three, scale the foundations. Roll out the registry statewide. Open district care coordination offices. Train the first cohort of Dementia Supporters. Pilot the Fund in two or three districts. Begin the Age-Friendly Panchayat certification. Open memory clinics in every district hospital.
In years four through ten, the system matures. The Fund expands towards broader coverage. The caregiver workforce reaches scale. The dementia ecosystem becomes a recognised model. The panchayat-level system becomes the operational backbone, the state-level system the regulator and financier of last resort.
This sequence needs political continuity that no policy can guarantee. The Department's design should therefore include sufficient legislative grounding, institutional independence, and ring-fenced financing to withstand changes in government. It should not depend on the goodwill of any one Chief Minister or Finance Minister to keep functioning.
And, to state the obvious because it is often overlooked, the Department is a beginning, not an end state. Kerala's ageing demographic will demand Ministry-level political attention by the early 2030s.
The recommendation of this paper is that the Department be treated as the first phase, with an explicit commitment, built into its founding documentation, to review its institutional status within five years. What is created now should be designed to be upgraded, not merely to survive.
A test, not a crisis
Kerala's ageing is often described as a crisis. It is more honest to call it a test. The state's earlier achievements gave its people longer lives. The test now is whether we can give those longer lives the dignity, function, and connection that make them worth living.
A well-designed Department cannot do this alone, but it can take the question seriously and organise the government and the wider ecosystem around it. The Department has been formed. The Government Order has been issued. Kerala is the first state in India to take this step, and other states are watching. The question is no longer whether to act, but how to use the next 60 months, the window in which the Department must either prove its reach or make the case for elevation to the full Ministry.
Kerala has done difficult things before. The literacy mission, the decentralisation that gave panchayats real powers, the palliative care movement that began in Kozhikode and went global: each of these started with the state organising around a hard question that the rest of the country was avoiding. Ageing is the next question.
The woman in Pathanamthitta is unlikely to read this paper. The Department that will decide how she spends her next ten years has just been created.